Dr. Anita Tamang Waiba, MBBS
Passionate and enthusiastic medical graduate with an experience of serving rural communities in Nepal since 2021. Adept at delivering top quality care with energy and competence, always treating patients with empathy, kindness and compassion. Eager to expand my knowledge and expertise in the medical field. Outside of work, I enjoy exploring my love for photography and traveling.

Medical Education & Training
- Clinical Medicolegal (MoHP, Nepal)
- How to Write and Publish Scientific Research Papers (PAHS)
- Training on Clinical Research (JNMA)
- S. T. A. B. L. E. (PAHS)
- Palliative Care Course (PAHS)
- Critical Care Training for Health Care Workers for the Management of COVID19 (NHTC Nepal, WHO, NMA)
- Let's Break the Chain of COVID19 Infection (MRBU)




- Advanced Skilled Birth Attendant (NHTC, Nepal): performed more than 120 solo C-sections including repair of uterine rupture
- Essential Critical Care (NHTC, Nepal)
- Kangaroo Mother Care (PHTC, Nepal)

- Risk Communication and Community Engagement (PHTC, Nepal)
- Human Rights and Medical Ethics Related to HIV (PHTC, Nepal)
Trainer
Ambulance Driver Training - 1st batch, Gandaki Province
First Aid Training to Nepal Police, Myagdi District





Clinical Experience
Ophthalmic Assistant
At Tilganga Institute of Ophthalmology: Full time
Worked as a scrub assistant in cataract surgery, oculoplastic surgeries and vitreo-retinal surgeries.
At Global Eye Center: Part time
Worked as a scrub assistant in oculoplastic surgeries.
Medical officer
At District Hospital, Taplejung: Full time
Provided outpatient care, emergency care, inpatient care, point of care ultrasound service, obstetric scan, maternity service including emergency cesarean section, one - stop crisis management(OCMC), and medicolegal services.
COVID-19 management
At Beni Hospital, Myagdi: Full time
Provided outpatient care, emergency care, inpatient care, point of care ultrasound service, obstetric scan, non communicable disease prevention program, OCMC, and medicolegal services.


Developed Tool
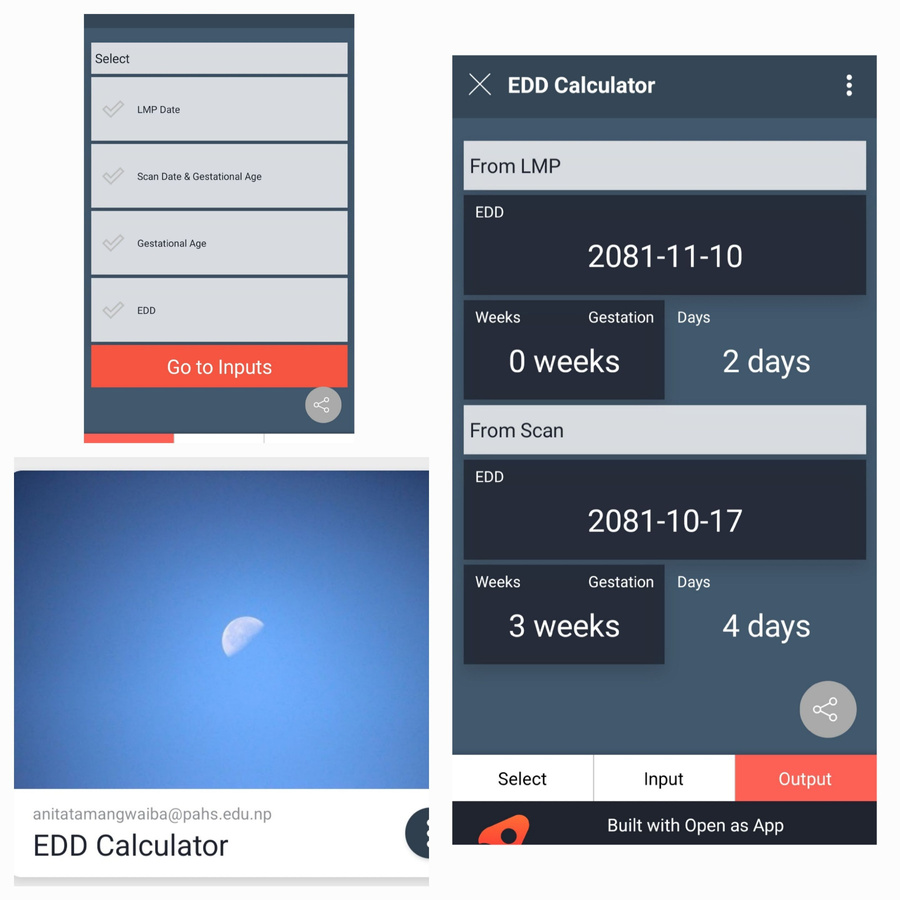
This tool is developed to calculate gestational age, expected date of delivery using Bikram Sambat calendar (official calendar used in Nepal).
This helps to minimize error of EDD and gestational age calculation.
Publications & Research
Volunteering Activities

Free Health Camp, Galeshwor Elderly Home, Myagdi

Free Health Camp organized by Beni Hospital & Nepal Army at Chimkhola, Raghuganga, Myagdi
Conference


Oculoplastic Conference in Universitas Gadjah Mada, Indonesia 2015
Conference



BLOGS
BLOG 1: A story inside Pasupati Elderly home
2 PM, I entered from the east gate of Social Welfare Centre Elderly’s Home, Pashupati.
Surrounded by long houses, there are five white temples above the stairs on four sides. Social Welfare Centre Briddhashram is the only elderly's home operated by the government of Nepal. It was established in 1882 A.D as Panchadeval Pakshala. It is giving shelter up to 230 persons.
To get shelter in this home, applicant must be a Nepali citizen with age above 65. A recommendation letter from the concerned Village Development Committee or Municipality is required, stating that the person is helpless, poor and has nobody to take care of. The concerned person should submit an application to the Ministry of Women, Children and Social Welfare requesting for permission to live in Elderly's Home.
During the observation, a voice of an elderly woman was heard – “Why had you come when it is raining? You could have come on other days. You can get fever from rain.” Those words full of love belonged to an elderly woman with bright, lively face who was talking to us. “Aama, are you fine?” I asked. “I am alright”. I handed over the fruits that I had brought for her. “Why did you have to bring all these? Please bring very little from now.” She took me to her room and offered some curd, “Relation should be both-sided not one-sided.” She started taking out different sweets, biscuits and juice for me. “Donors keep on bringing all these things. I can’t finish them all.”
Now 81, she was married at the age of 13. She was taught to read and write by her father. Her husband used to work in India. She said that she used to read her husband’s letter all night. After her only daughter died at the age of 3 months, she didn’t have any other child. Her husband married another girl in India and stayed there. Once, she got a chance to Satsang discourse. The discourse influenced her to stay away from the worldly desires. She came to the conclusion that marriage is a worthless relationship that takes away independence. She went to Devghaat Elderly Home, near Narayangadh at the age of 70. Due to intense heat, she couldn’t stay there for long. After three years, she moved to Social Welfare Center Elderly Home Pashupati. It has been seven years now. She thinks she is happy here, she can eat what she likes such as dahi, mohi (curd and lassi).
She is taking medicine regularly for gastritis and hypertension. Other elders staying there also have different health problems. Unlike her, many have problems in their joints. Talking about her condition she says, “In the shade of God, I am very happy. My only wish now is that I could die without being disabled.” In weekly health checkups, blood pressure and other minor health problems are checked. For minor problems, medicine is provided there whereas for major problems, they are taken to hospital. The elders are given food three times a day. Besides that, people and organizations coming from outside also distribute food to them.
Aama said that the staffs working there come only at days but during night, there is no one to take care of them. ‘Mare faalne, baache paalne’, if we die they throw away and if we live they feed us, they work in this way, said aama in a bit sadder tone. Although it is said that elderly people are hard to please, I felt that it might be due to the lack of good rapport between the elderly people and the staffs working there.
She has relatives, but they don’t care much about her. “Why should I belittle myself by going to them?” she talked of dignity. She hugged me, caressed my hands and said “Please come time and again, will you?” She treated me as her own daughter.
Blood relation is the relation of duty. Some fulfill their duty whereas others deviate away from their duty. Relation of sentiments is hard to create, but once established it is more powerful than the relations of blood. Love gives us the power to face and tackle the challenges that come in every step of our life. Thus, love is the greatest virtue. Even with the stranger she just met she talked so sweetly, such is her love.
Those same children who were fed, clothed by their parents, their small hands and legs that were oil massaged by their mothers, how can they abandon the same old parents? Why do they hate them? Did God deliberately filled humanity only in some of the people and not in others? When people get old and they can’t work anymore, they are often forced to leave home even by their own children. This indicates that we are getting more materialistic and less spiritual. We must not be too mechanical. It would be better to use our heart and mind for happy life.
BLOG 2: च्यातिएको पाठेघरको जटिल शल्यक्रिया जिल्ला अस्पतालमा गर्दाको क्षण
पाटन अस्पतालबाट एमबिबिएस सकिएपछि मेरो जागिरे जीवन २०७८ श्रावण ८ गतेदेखि जिल्ला अस्पताल ताप्लेजुङमा सुरु भयो।
भाद्र महिनामा मिक्वाखोला गाउँपालिकाबाट वर्ष ४५ को “क” नाम गरेको बिरामी उहाँको श्रीमानसँग ओपिडिमा आउनु भयो। महिनावारी टाइममा नभएको र मेडिकलमा पिसाब जाँच गर्दा गर्भवती देखिएको भएर गर्भपतन गराउने भन्नु भयो। महिनावारी नियमित नहुने भएकोले गर्दा कति हप्ताको गर्भ हो यकिन गर्न सकिएन। अल्ट्रासाउन्ड गरेर हेर्दा २२ हप्ताको गर्भ देखियो। कानूनी रूपमा गर्भपतन गराउन मिल्दैन भनेर परामर्श दिएँ, त्यसपछि उहाँहरू निस्किनु भयो।
यस बीच कार्तिकको अन्तिम देखि माघ सम्म NSI बाट ASBA तालिम लिने मौका पाएँ। मेरो तालिम भरतपुर अस्पतालमा थियो जहाँ exposure मनग्य हुन्थ्यो। सुरुको २ हप्तामा अवलोकन र सहयोग (assist) मात्रै गरेर पनि ७० दिने तालिममा ९० ओटा जति cesaean-section (अपरेशनबाट बच्चा जन्माउने) गर्न पाएँ। तालिम पश्चात् ताप्लेजुङ जिल्ला अस्पतालमा cesarean-section अपरेसन सुरु गरें। मभन्दा पहिले NSI को अपरेसन गर्ने डाक्टर हुनुहुन्थ्यो, तर म गएको ३/४ दिन पछि उहाँको पनि सरुवा भयो। अब त्यहाँ अपरेसन गर्न म एक्लै थिएँ। विषेशज्ञ डाक्टर नभएका कारणले काम गर्दा धेरै नै सोच विचार गरेर मात्रै बिरामीलाई उपचार परामर्श दिन पर्ने हुन्थ्यो। ताप्लेजुङबाट रिफर गरी झापा पठाउन ८/९ घण्टा लाग्छ। रिफर गरेर पठाउँदा पनि धेरै जटिल अवस्था को बिरामी बाँच्ने सम्भावना धेरै कम हुन्छ। हामीले परामर्श पनि त्यही अनुसार गरेर पठाउने गर्छौं।
२०७८ चैत्र ५ गते एकजना व्यक्ति आफ्नो गर्भवती श्रीमतीलाई प्रसूति गराउन लिएर आउनु भयो। उहाँको यो छैठौँ गर्भ अवस्था ३७ हप्ता ६ दिन पुगेको र सुत्केरी व्यथा सुरु भएकोले भर्ना गरेर राखियो (G6P5L5)। उक्त बिरामी भाद्र महिनामा गर्भपतन गराउन खोज्न आउनु भएकै बिरामी हुनु हुँदो रहेछ, श्रीमान चाहिँ प्राथमिक विद्यालयको शिक्षक। धेरै पटक गर्भ भएको कारणले यो बच्चा जन्माउने क्रममा जटिल समस्याहरु आउन सक्छ, अपरेसन गर्न पर्ने अवस्था आउन सक्छ, विषेशज्ञ डाक्टर भएको अस्पतालमा रिफर भई जान अनुरोध गरेपनि उहाँहरूले ५ वटा बच्चा घरमै जन्माएको हो हामी जे जस्तो पर्छ यो बच्चा यही नर्मल जन्माउन कोसिस गर्छौं, अपरेसन गर्न परे पनि तपाईंसँगै गराउँछौं, झापा पुग्न टाढा अनि पैसा बढी लाग्छ भन्ने कुरा गर्नुभयो। भोलिपल्ट चैत्र ६ गते दिउँसो १२ बजे नै पाठेघरको मुख पुरै खुलिसकेको (cervical os fully dilated) भएको तर १:३० सम्म पनि delivery नभएको (बच्चा नजन्मिएको) कुरा नर्सले जानकारी गराउनु भयो। pervaginal examination गर्दा बच्चाको टाउकोअलि माथि नै भएको कारणले vacuum लगाउन सकिने अवस्था थिएन, एकैछिन पेटमा बल लगाएर (fundal force) दिएर vaginal delivery गराउन कोसिस गरियो, तर delivery नभएको हुनाले अपरेसनको तयारी गर्न थालियो। ताप्लेजुङ जिल्लामा ब्लड बैंक नभएको कारणले ब्लड डोनर खोज्न थालियो। करिब ४ बजे बल्ल बिरामीलाई अपरेसन कक्षमा सारियो। लठ्याउने सुई ढाडमा (spinal anesthesia) दिने बित्तिकै बिरामीको रेस्पोन्स कम भएको हुनाले, एनेस्थेटिक असिस्टेन्टले कृत्रिम श्वास (bag and mask) दिँदै गर्दा, मैले तुरुन्तै अपरेसन सुरु गरेँ। पेट (peritoneum) खोल्ने बित्तिकै पाठेघर बाहिरै रगत (blood )देखिन थाल्यो, पाठेघर च्यातिएर बच्चा त पाठेघरबाट निस्केर पेटमा (abdominal cavity) मा रहेछ। त्यो बेलामा अस्पतालमा जम्मा २ जना डाक्टर थियौँ, दुवै जना मेडिकल अधिकृत। मैले पाठेघर च्यातिएको (uterine rupture) त्यो भन्दा पहिला कहिल्यै देखेको थिइनँ। झटपट एकजना स्टाफलाई कुदेर अर्को डाक्टरलाई बोलाउन पठाएपछि उहाँले आएर बच्चालाई resuscitate गर्न थाल्नु भयो। दुर्भाग्यवश, बच्चालाई बचाउन सकिएन। अपरेसनमा धेरै समय लागेकोले, बीच बीचमा बिरामीको श्रीमानलाई भित्र के भइरहेको छ भनेर जानकारी दिइरहेको थियौँ। मेरो बुद्धिले भ्याएसम्म मैले च्यातिएको पाठेघर (ruptured uterus) लाई सफा गर्ने सिलाउने (repair) गरी पेटबाट फोहोर बाहिर निस्कियोस् भनेर पेटमा पाइप (intra-abdominal drain) राखेर post-op मा मनिटरमा (cardiac monitor) मा राखियो, रगत चढाउने (blood transfuse) पनि गरियो।
भोलि हेर्दा फोहोर पानी आउने झोला (drain bag) मा फोहोर पानी (fluid collection) थिएन तर पाइप (drain tube) काे बाहिरबाट भने पानी (fluid) निस्किरहेको थियो। पाटनमा कार्यरत सहकर्मीसँग सल्लाह लिँदै, उपचार गर्दै गयौं, बिरामीको शरीरमा प्रोटिन कमी देखिएकोले झापाबाट अर्डर गरेर प्रोटिन (albumin) दिँदै बिरामीको अवस्था सुधार हुँदै गयो। करिब ७ दिनको अस्पताल बसाई पछि बिरामी डिस्चार्ज हुनु भयो।
देशकै ठूलो अस्पतालका प्रसूति डाक्टरहरुलाई पनि यस्तो अपरेसन गर्न र बिरामीको ज्यान जोगाउने काम निकै चुनौतीपूर्ण कुरा हो। जिल्ला अस्पतालमा जहाँ बेहोस पार्ने डाक्टर, ब्लड बैंक, अनि दक्ष प्रसूति डाक्टरको अभावमै पनि एकजना बिरामीको ज्यान जोगाउन सक्नु हामी जिल्ला अस्पतालको टिमको लागि एउटा विजयको कथाको रूपमा मैले लिएको छु। यो मेराे जीवनको अविस्मरणीय क्षण रहनेछ।
अन्त्यमा, दुर्गम ठाउँ जहाँ १/२ जना डाक्टरको भरमा जिल्ला अस्पताल चलाउन पर्ने बाध्यता, ब्लड बैंक नभएको कारणले जति नै इमर्जेन्सी अपरेसन भने पनि ब्लड ग्रुप मिल्ने मान्छे खोज्न पर्ने अवस्था, टाढा रिफर सेन्टर, र विषेशज्ञ चिकित्सक नहुने ठाउँमा विभिन्न तालिम प्रदान गरी नेपालको मातृशिशु स्वास्थ्यमा अमूल्य योगदान प्रदान गरी दूर दराजमा रहेका परिवारहरुको जीवनमा हुन सक्ने अपूरणीय क्षतिलाई रोक्ने क्षमता राख्ने, NHTC, Nick Simon's Institute, जिल्ला अस्पताल ताप्लेजुङ लगायतका निकायहरुलाई हृदयदेखि धन्यवाद।

Get In Touch
Email
anitawaiba@gmail.com
Social